
Surgical Techniques
In surgery, the goal is to give our patients the best outcomes for survival and quality of life by removing as much of the tumor as possible, while protecting critical sites of sensory, motor, and cognitive function.
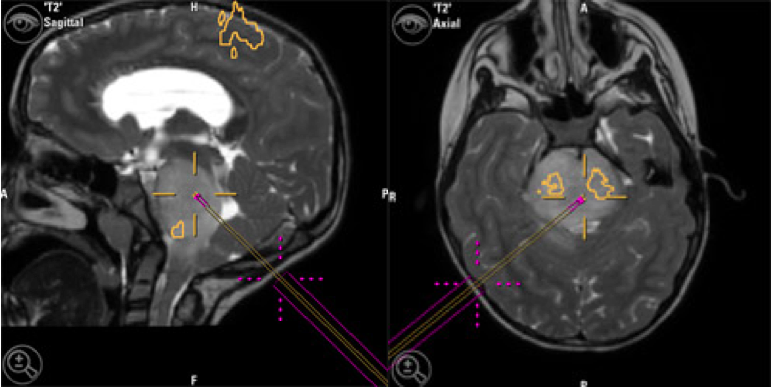
Neuronavigation systems are computer-assisted technologies that provide neurosurgeons with better visual feedback during surgery. It is like having a GPS or Google Maps for a neurosurgeon to navigate their patient’s brain. To create a custom “map” for each patient’s brain, these systems use scans collected from the patient before surgery (like high resolution MRI). The preoperative scans are useful for visualizing anatomical landmarks in the brain, as well as the location and extent of the tumor. Intraoperative imaging during the surgery shows where the surgeon’s instruments or probes are within the patient’s brain, in addition to certain neural and vascular structures. By overlaying these images, neuronavigation provides a more detailed, live map for surgeons to make visually guided movements.
Using neuronavigation systems, surgeries can be simulated and planned ahead of time, allowing for maximum accuracy. As a result, mistakes in trajectory and depth during tumor resection are prevented. In addition, the shortest and safest route can be selected that avoids important neural and vascular structures. Surgeons combine “functional” and anatomic information obtained from preoperative imaging with neuronavigation to help find the safest route. This process, called “functional neuro-navigation”, reduces the risk of postoperative neurologic deficits and improves assessment of risk beforehand. Specifically, it allows for accurate localization of the tumor, and enhances the extent of tumor removal; this both improves safety for the patient and improves their outcomes with greater tumor resection. With all these advantages, neuronavigation systems are used for most neurosurgical procedures.
During an operation, a neurophysiologist monitors electrical signals in the patient’s brain, cranial nerves, and spinal cord to make the tumor removal as safe as possible. This process is called intraoperative neuromonitoring (also called intraoperative neurophysiological monitoring, or IONM).
Intraoperative neuromonitoring uses a variety of methods to locate and monitor specific brain regions and nerves. This helps the surgeon remove as much of the tumor as possible, while protecting important function in the neighboring tissue. Depending on the location of the tumor and the specific brain regions at risk, different combinations of the following techniques may be used:
Somatosensory Evoked Potentials (SEPs or SSEPs)
During surgery, SSEPs are monitored to protect the brain regions that control a patient’s sense of touch.
An SSEP is the electrical activity in the brain that results from sensory stimulation on the body. SSEPs have a characteristic electrical pattern that is reliably identified across different parts of the brain. For example, a touch stimulus (like from a pin prick or puff of air on the finger) will evoke measurable voltage peaks at precise times in the brain regions responsible for body sensation, including a voltage peak in the somatosensory cortex at 60 milliseconds after the stimuli, and another voltage peak in the parietal cortex at 100 milliseconds after the stimuli. Neurophysiologists can identify critical brain regions based on the precise pattern of electrical activity recorded.
Throughout the surgery, the neurophysiologist applies small electrical pulses to specific sensory nerves that carry information from the body to the brain. Like a touch stimulus, this initiates subsequent electrical activity in the corresponding areas of the patient’s brain. The neurophysiologist locates and monitors SSEPs in the brain to help the surgeon avoid the sensory processing regions.
Motor Evoked Potentials (MEPs)
During surgery, MEPs are monitored to protect the brain regions that control a patient’s ability to move (motor function).
An MEP is the electrical activity in muscles that results from applying small electrical currents to motor regions of the brain. A neurophysiologist can locate and monitor these brain regions by electrically stimulating the brain surface, and looking for the subsequent electrical activity, or MEPs, in specific muscles. This type of neuromonitoring is vital for surgical removal of tumors near brain regions that control motor function.
To measure MEPs, ‘recording electrodes’ are placed on different parts of the patient’s body (like their arms or legs). ‘Stimulating electrodes’ are placed on the surface of the brain, to test brain tissue for motor function. A computer system that is connected to the stimulating and recording electrodes initiates the electrical stimulation in the brain, and milliseconds later, precisely records the subsequent electrical activity in different parts of the body.
Throughout the surgery, the neurophysiologist applies small electrical pulses to the brain and monitors for electrical activity in the corresponding muscles along the patient’s body. For example, if stimulating an area of the brain evokes an MEP in the patient’s hand, then that area is protected during the surgery. This helps the surgeon avoid motor regions of the brain, so the patient’s ability to control body movement is preserved.
Nerve Conduction Studies (NCS)
NCS are tests that evaluate how well specific nerves are functioning. One of the measures collected is the speed at which electrical signals are transmitted (or conducted) along a nerve.
For example, a motor nerve normally transmits electrical signals to a muscle, causing it to contract. During motor NCS, small electric currents are applied to a motor nerve via a ‘stimulating electrode’. ‘Recording electrodes’ on the muscles record the corresponding electrical response, while a computer system measures the time delay between electrical stimulation of the nerve, and the subsequent electrical response in the muscle. With this information, the neurophysiologist can determine how quickly electrical signals are transmitted by a motor nerve, which is a sign of how well the nerve is functioning.
During surgery, NCS helps monitor the function of critical nerves, preserving important sensory and motor nerves that may be near the tumor site.
Electromyography (EMG)
EMG is a technique for recording electrical activity in muscle cells. It is the diagnostic technique used to record muscle responses during motor mapping, motor NCS, and MEP tests. This is done by placing electrodes on the surface of the skin, or by inserting a thin electrode directly into the muscles.
The purpose of motor mapping, motor NCS, and MEP tests is to protect and identify motor regions of the brain that transmit information to control specific muscles. Each of these techniques involves applying electrical stimulation to the brain regions surrounding the tumor. EMG is what neurophysiologists use to measure and record subsequent electrical activity in the relevant muscles. This helps determine which brain areas near the tumor need to be preserved.
Electroencephalography (EEG)
EEG is a technique for recording electrical activity in the brain. This is done by placing electrodes on the scalp that can detect broad changes in electrical patterns in the underlying brain. Because anesthesia causes certain characteristic changes to brain activity, EEG is used to monitor and maintain proper levels of anesthesia for the patient. Sudden changes in cerebral blood flow can also affect EEG readings, so EEG is used during surgery for monitoring blood flow in the brain.
Intraoperative magnetic resonance imaging (intraoperative MRI) provides surgeons with real-time, high-resolution images of the brain during surgery. This provides accurate information during the surgery, especially since the brain can shift as tissue is removed. Further, intraoperative MRI can help confirm whether a tumor has been fully removed.
Like MRI that is performed prior to surgery, intraoperative MRI uses magnetic fields and measures radio waves to produce an accurate image of a patient’s brain, including identification of abnormal tumor tissue. Available at UCSF, intraoperative MRI involves specialized, advanced equipment that allows MRI to be taken during a surgical procedure.
Intraoperative computed tomography (intraoperative CT) provides surgeons with real-time images of the brain during surgery. This helps provide accurate information during the surgery, especially since the brain can shift as tissue is removed.
Like CT scans that are taken prior to surgery, intraoperative CT uses a series of X-ray measurements taken from different angles to generate an image of a patient’s brain that includes certain anatomical landmarks. Intraoperative CT involves specialized equipment, like the Brainlab Airo system used at UCSF, which allows CT scans to be taken during a surgical procedure.
This content was reviewed by UCSF neurosurgeons, Mitchel Berger, MD and Shawn Hervey-Jumper, MD.