
Maximizing Tumor Resection Improves Low-Grade Glioma Patient Outcomes
UCSF Brain Tumor Center Researchers Define Thresholds for Extent of Resection
Adults with low-grade glioma can live longer if neurosurgeons remove as much of the brain tumor as possible, according to a new study led by researchers at the UCSF Brain Tumor Center.
Since the World Health Organization’s 2021 reclassification of diffuse gliomas based on the tumor’s molecular features, researchers have been questioning how much different glioma subtypes benefit from extensive tumor resection.
The findings now represent a paradigm shift in the management of low-grade malignancies, particularly for oligodendrogliomas, says the study’s co-senior author Annette Molinaro, PhD.
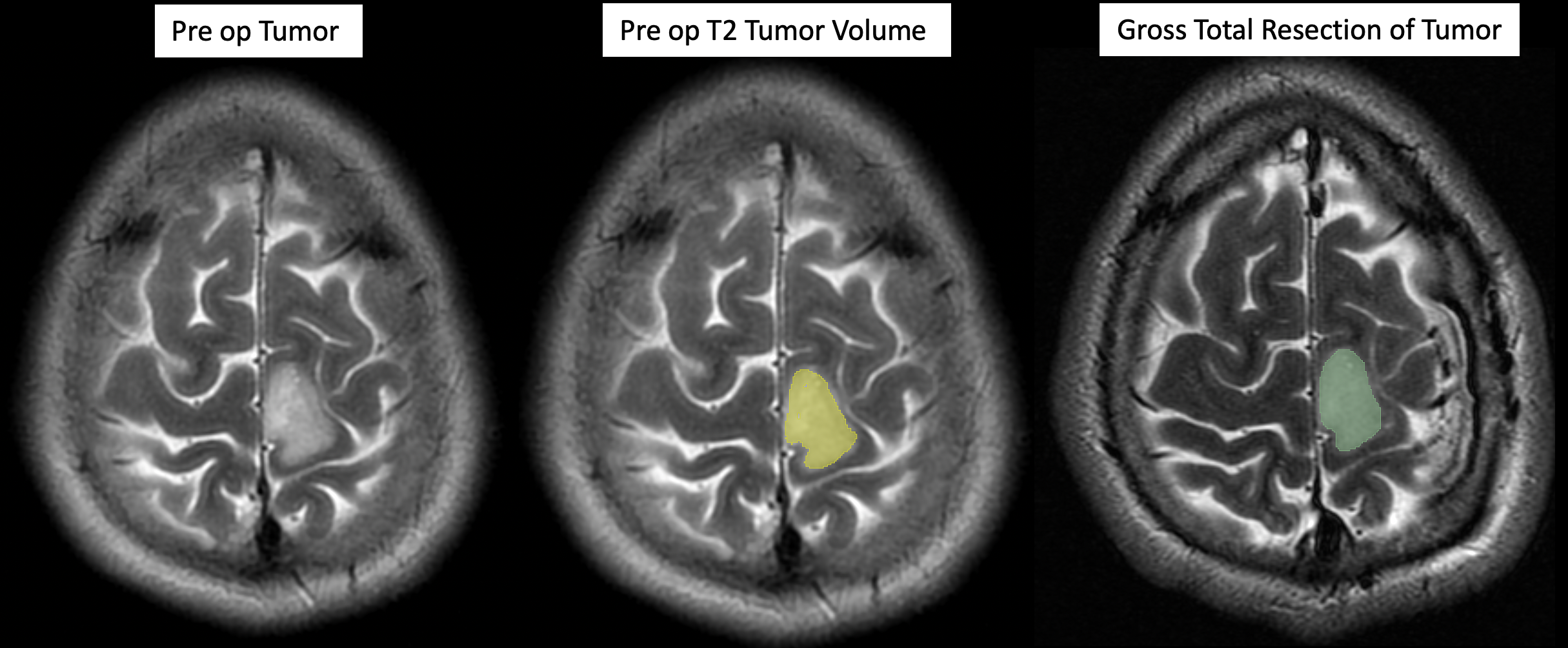
The study, published January 4 in the Journal of Clinical Oncology, tracked the outcomes of 392 patients with IDH-mutant grade 2 glioma who were initially diagnosed and treated at UCSF between 1998 and 2017. Neurosurgery residents Ramin Morshed, MD, and Jacob Young, MD, looked at all the MRIs from the patients 24 hours before surgery as well as within 48 hours after surgery, to calculate the tumor volumes and extent of resection.
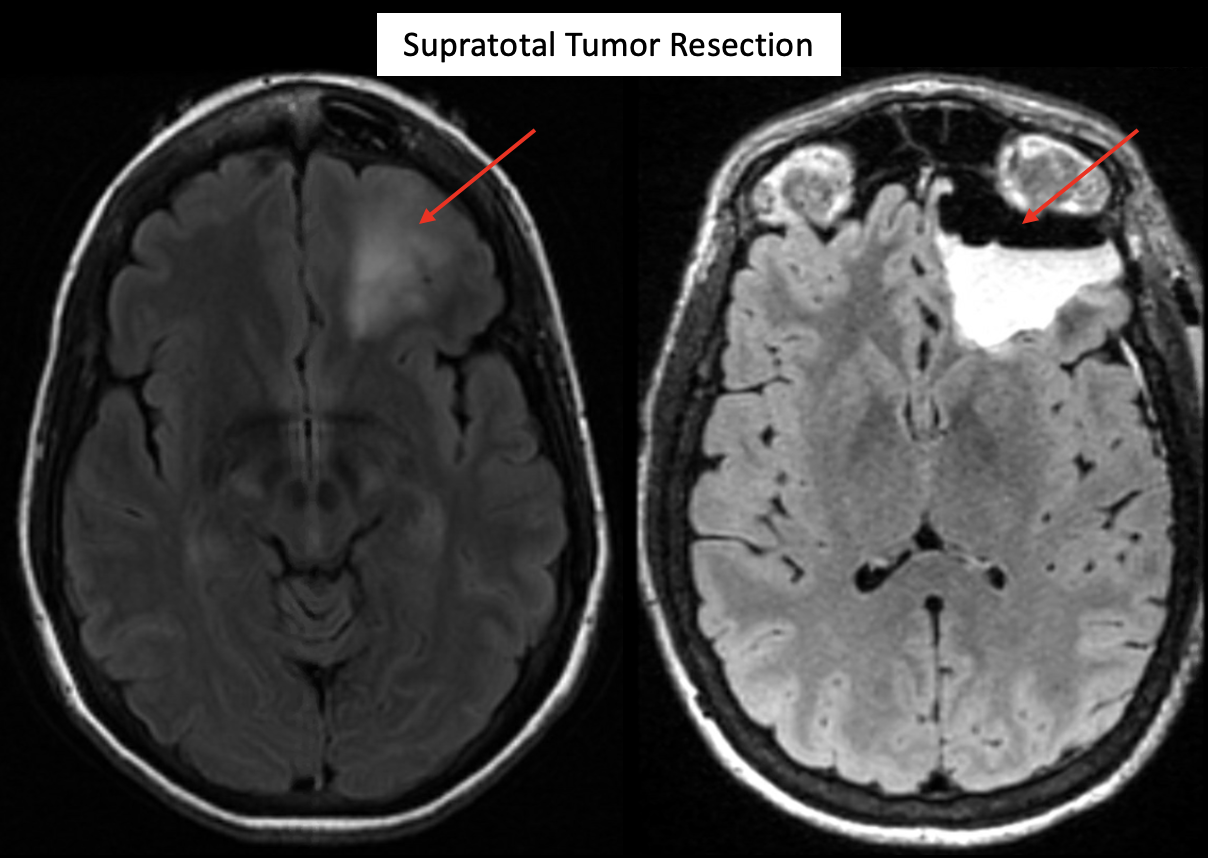
The researchers then grouped the resections into three categories based on the amount of tumor remaining following surgery. Gross total resection (GTR) indicated that the surgeons had removed all the tumor visible from the brain scans. Patients in the GTR plus group received a supratotal resection – meaning that the neurosurgeons went beyond the margins of the tumor defined by the MRI.
In high-grade disease, several research groups – including at the UCSF Brain Tumor Center – have shown that safely resecting non-contrast enhancing tumor increases survival for glioblastoma patients. Senior co-author and UCSF Brain Tumor Center director Mitchel Berger, MD, says this study now shows that neurosurgeons can also extend survival for low-grade glioma patients with a more aggressive resection.
“If we go beyond the margin of the tumor, we can reduce the risk of malignant transformation,” he said. “This is a huge victory for patients with low-grade gliomas.”
The survival benefit of removing non-contrast enhancing tumor was more pronounced in astrocytomas, but Molinaro, who is also the director of the Division of Biomedical Statistics and Informatics for the UCSF Department of Neurological Surgery, says their results still point to the importance of resecting 100 percent of oligodendrogliomas.
“A huge advantage of our study is that we followed these patients for so long,” Molinaro said. “It's around 10 years that we start to see that the amount of tumor resected makes a difference.”
The analysis identified three patient risk groups based on tumor subtype as well as the pre- and post-operative tumor volumes. For both oligodendrogliomas and astrocytomas, leaving less than 4.6 milliliters of tumor results in better patient outcomes.
Through a collaboration with Brigham and Women’s Hospital in Boston and with St Olavs University in Norway, the researchers also demonstrated in a combined cohort of 757 glioma patients that overall survival was significantly better in those who had more than 75 percent of their tumor resected.
“Residual tumor volume or percent resected should be included as a stratifier in therapeutic clinical trials, similar to age and IDH mutational status,” Molinaro said.
UCSF neurosurgeon and first author of the study Shawn Hervey-Jumper, MD, notes that surgical resections should maximize the amount of tumor removed while preserving post-operative neurologic function.
"The whole reason that we can have this conversation is because there have been a number of techniques like functional brain mapping and imaging that have been perfected to try to remove the tumor without hurting the patient,” Hervey-Jumper said.
Paper(s) cited:
Hervey-Jumper SL, et al. Interactive Effects of Molecular, Therapeutic, and Patient Factors on Outcome of Diffuse Low-Grade Glioma. J Clin Oncol. 2023 Jan 4:JCO2102929. doi: 10.1200/JCO.21.02929. Epub ahead of print.